What are the Symptoms?
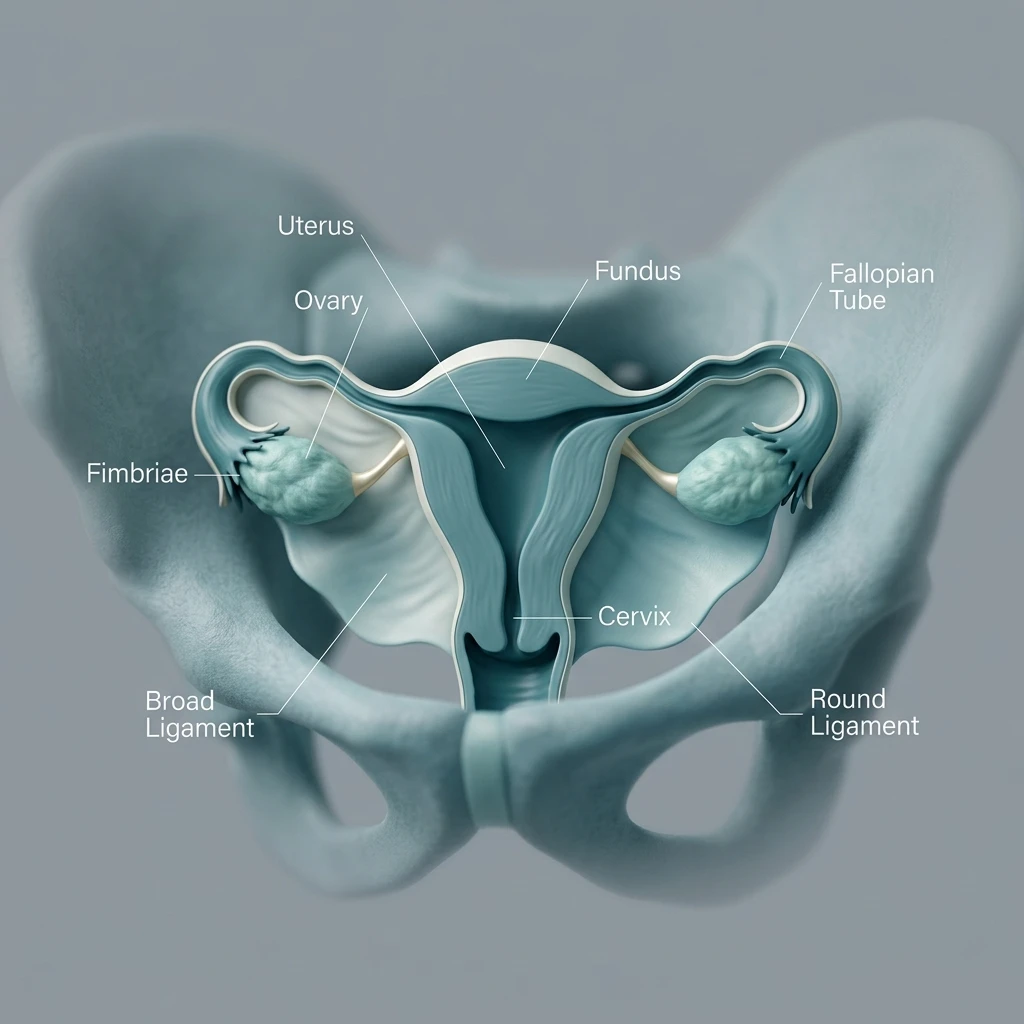
It can primarily occur in the lower abdomen, ovaries, and fallopian tubes, as well as in many other areas including the bowel, diaphragm, nerves, and thoracic cavity. Although endometriosis is a common and benign condition, the cellular changes resulting from endometriosis can lead to the following symptoms:
- Dysmenorrhea and menstrual pain unresponsive to analgesics
- Dyspareunia
- Chronic pelvic pain
- Pain during defecation or urination (Dyschezia or Dysuria)
- Bouts of diarrhea-constipation
- Posterior leg-lower back pain and chronic fatigue
- Infertility
- More rarely, hematemesis and right shoulder pain
The severity of these symptoms can vary from person to person and may worsen, especially during menstruation.
How Does It Occur?
Although this topic is not yet fully clear, in endometrioma, endometrial cells pass through the fallopian tubes and implant on organs within the abdominal cavity. While most women can clear these cells from their bodies, it is thought that there is a defect in this mechanism in patients with endometriosis.
Apart from this theory, it is also believed that cells present from birth differentiate into endometriomas over time. The cellular differentiations that occur result in chocolate-colored cysts containing blood products in the ovaries and formations called firm nodules in other organs.
How Many Types Are There?
Endometriosis lesions can be categorized as superficial, affecting the peritoneal lining, or deeply infiltrating, affecting the bowel, ureters, bladder, and uterine ligaments. Additionally, they can be divided into 4 stages—mild, moderate, and severe—depending on the affected organ and the extent of the disease.
- Ovarian endometrioma (chocolate cyst): Forms due to the implantation of endometrial cells within the ovary, containing dark brown cyst fluid. It can be bilateral.
- Deep (advanced stage) endometriosis: Frequently involves the peritoneal lining, uterine ligaments, bowel, bladder, nerves, ureters, diaphragm, lungs, and other pelvic organs such as the vagina.
Who Is More Commonly Affected?
Factors associated with an increased risk of endometriosis include: nulliparity, early menarche, late menopause, short menstrual cycles, congenital organ anomalies, family history of endometriosis, tall stature, high consumption of trans unsaturated fats, and living in an industrial area.
How Is It Diagnosed?
Physical examination findings: Tenderness on vaginal examination, palpable nodules, and rarely, visualization of endometriosis involvement in the cervix or vaginal tissue. The absence of these findings does not rule out the disease.
Blood test: There is no definitive laboratory test for diagnosing endometriosis. Serum CA 125 levels may be elevated, but routine testing in all patients is not recommended.
Radiological tests: Transvaginal or abdominal ultrasound is usually sufficient for diagnosing endometrioma. In some cases, contrast-enhanced lower abdominal MRI may also be used for diagnosis.
Treatment Options
Analgesics
These may be preferred in patients whose primary complaint is pain, especially during menstruation. In endometriosis treatment, they are used only for symptom suppression and have no role in definitive treatment.
Progestin-containing Medications
These can be used in patients with predominant pain complaints and may partially reduce pain. Progestin-releasing intrauterine devices (IUDs) can be used in patients with uterine involvement.
Oral Contraceptives
For endometrioma patients experiencing menstrual irregularities or pain during progestin therapy, continuous use of oral contraceptives may be recommended.
GnRH Agonists (Temporary Menopause Inducing Injections)
These medications suppress estrogen hormone levels, creating a temporary menopausal state in patients. This condition resolves after the medications are discontinued. Due to the risk of osteoporosis, use for more than 6 months is not recommended.
Laparoscopic Surgery
Laparoscopy is a method where surgical instruments are used through 3-4 small incisions made on the abdominal skin to visualize the abdominal cavity and, if necessary, excise endometriotic foci. Surgical treatment is particularly required in cases unresponsive to medical treatment, persistent pelvic pain affecting daily quality of life, presence of large, suspicious-looking ovarian cysts, bowel and bladder involvement, risk of kidney loss due to ureteral involvement, pulmonary involvement, and nerve involvement.
The success of laparoscopic treatment depends on the size of the mass, involvement of both ovaries and the uterus, completeness of the surgery, and the surgeon's experience.
Endometrioma and Ovarian Reserve
Adolescent girls have approximately 400,000 eggs. As age advances, the egg pool begins to diminish. Conditions like endometrioma accelerate the rate of this reserve depletion. Furthermore, there is data suggesting that it impairs the quality of existing eggs.
Ovarian reserve is determined by an FSH test performed on the 3rd day of menstruation, ultrasound follicle count, or a blood AMH test.
Endometrioma and Desire for Children
Infertility rates in women with endometrioma are approximately 30-40%. The reasons for this include adhesions within the abdominal cavity or fallopian tubes, decreased ovarian reserve, reduced egg quality, disruption of the suitable environment for embryo implantation by fluids released from the cyst, prevention of egg-sperm fusion, and prevention of embryo implantation in the uterus.
Patients with bilateral cysts, a history of ovarian surgery, those over 35 years old, and those with low ovarian reserve test results who desire children should absolutely consider egg or embryo cryopreservation options before surgery.
Endometriosis During Pregnancy
During pregnancy, endometriosis lesions may sometimes regress in response to the changing hormonal environment. However, this does not completely suppress the lesions. If pregnancy occurs in the presence of endometrioma, miscarriages, preeclampsia, preterm birth, and placental adhesion abnormalities can rarely be observed.
Endometrioma and Cancer
Although endometrioma can rarely be associated with cancers, the overall risk appears low. According to one study, this risk appears to be around 2.56% in the general population, with a lower risk before the age of 40 (1%) and a slightly higher risk in patients over 40.
All Specialties